The known unknowns
The recent outbreak of the Delta variant led to a number of unintended consequences. Growers dumped thousands of flowers they weren’t allowed to sell. Auckland factories producing construction materials were shuttered for five weeks. Deaths from influenza are at an all-time low. Now, New Zealand needs to decide how to manage COVID-19, based on incomplete information about its risks. Some of the most crucial metrics are ones we don’t have—such as how many people develop long-term illnesses. This is what we wish we knew.
It was a Saturday morning, January 18, 2020, and the man had stopped by Animates in Dunedin because he was worried about his dog. It was small and fluffy, like a Tibetan terrier, remembers veterinarian Sue Robb, and it hadn’t been eating properly since he’d picked it up from the boarding kennel. She told the man that his dog was probably just feeling disoriented after two weeks in a busy, noisy place.
Robb, who has been a vet for more than 40 years, has a solid, reassuring presence. Previously, she had worked as a kind of vet detective in Auckland, giving a second opinion on odd cases: people would bring her animals with mysterious health problems that other vets couldn’t figure out.
The man, overcome with gratitude, shook her hand, taking it in both of his. He’d just returned from somewhere near Wuhan in China, he said, and was relieved to be back in New Zealand. The city was closing down, and he’d thought he was going to get stuck there.
Robb started feeling sick three days later. She came down with all the usual symptoms of a cold, but it felt worse than any cold she had ever had, and she could never take a deep enough breath. She took a week off, but Animates was short-staffed, so she was pressured to head back. By now, she suspected that she’d contracted COVID-19. She knew that people overseas were having breathing difficulties—and her wife, who is asthmatic, had come down with it, too. She went back to work, and ordered an oxygen concentrator online.
Three or four months later, the illness came back with a vengeance, and this time, it was different. Pain in her muscles and joints. Intense fatigue, and a fog that descended in the middle of conversations, causing her to forget words. It was all Robb could do to drive to work and back without falling asleep. She and her wife spent hours a day hooked up to the oxygen machine, just breathing, too tired to do anything else.

Robb’s job didn’t allow her to reduce her hours, and her supervisors were frustrated with her reduced capacity. In November, she had a stroke. In January, she developed vasculitis in her legs: a painful inflammation of blood vessels. In February, she resigned from work. “My original plan was that I would keep going until I dropped dead,” she says, “because I really love my job.”
Robb, who is 67, is the kind of person who subscribes to medical journals for fun. At home—a caravan near Taieri Mouth—are ducks, guinea fowl, chickens, three cats, and a dog rejected by a local farmer for being unmotivated. Robb and her wife moved there three years ago to build a house, but the shortage of builders, their battles with COVID-19, and the loss of Robb’s income have got in the way. As this issue went to print, Robb was struggling to walk more than a few hundred metres from the caravan without the pain kicking in.
[chapter-break]
Geoff Brown agreed to MC the fiafia night at his daughter’s school on March 14, 2020, as a favour. As cases of COVID-19 ticked up in Auckland after the first, on February 28, other schools had been cancelling their events. But the evening was for a good cause, and his daughter would be performing with her Polyfest group.
A week later, Brown was making dinner—vegan chop suey—when a strange feeling came over his entire body. He went to lie down on the couch for a few minutes, leaving his daughter to continue cooking. When he woke up again, it was dark, and he was soaked through with sweat. He went outside, but the pre-dawn chill couldn’t cool him down. “If this is what I think it is,” he told himself, “I have to act fast.”
He got a camping mattress, a pillow, paracetamol, a cup, some teatowels and a lemon, and barricaded himself in the bathroom. He was determined to keep whatever he had away from his partner and three kids—they had to shout through the door to ask him how he was.

It felt as though he was deteriorating hour by hour. It became harder to breathe, and there was an odd pressure on his internal organs, and his heart started behaving strangely. “So my heart was, like, fluttery,” he says. “I’ve never had that before. My heart would flutter and stop and flutter and stop. It would freak me out.” Over the next few days, he tried, twice, to get a COVID-19 test, driving to a nearby testing centre with a teatowel tied over his face as a mask—“I became the Samoan Zorro”. He was turned away because he hadn’t been in contact with anyone who’d recently returned from overseas.
Finally, after five days on his bathroom floor, Brown called an ambulance. As the phone rang, he realised he didn’t know what to tell the paramedics, so he hung up. Instead, he called Healthline, then fell asleep waiting in the call queue. He was woken by a voice in his ear: “Hello, are you there? Hello?”
“Don’t hang up,” he croaked. “Don’t hang up.”
Before this, Brown had been feeling “amazing”. He’d gone plant-based over the summer, and lost weight. He was in the best shape he’d been in for years. “Nothing shut me down like this before, you know,” he says. “I’ve had pneumonia. I’ve been in trouble in my lifetime. I’ve been on the other side of life. I don’t fear many things.”


But when his wife drove him to hospital, teatowel tied over his face, he was nervous. He dipped into his rugby training. “I went into game mode. I told myself, I told my brain, I said, ‘Okay, whatever it does, I’m just gonna be ready.’”
He’d need that resilience over the months that followed. He tested positive for COVID-19 in hospital—“I thought to myself, ‘No shit, Sherlock’”—and during his stay, the illness loosened its grip on him. But it didn’t let go.
“So they call me recovered,” he says, remembering his return home from the first of what would become many visits to hospital. “I couldn’t even walk around. I couldn’t walk 20 metres without wanting to sit down and get a breather. I’m a former sportsperson. I was 48 years of age. And I’ll be honest with you, I’m still a tough bloke.”
[chapter-break]
Christina Orgias was laid low with COVID-19 for a little longer than a week at her flat in Manchester, where she was studying. She remembers the full-body muscle aches, so intense she took painkillers for them, and being left out of breath by a walk around the corner to pick up groceries. At least it was over quickly. But as she waited out her period of post-COVID isolation, unable to return to university, cities and borders around the world began to close. She caught the last flight out of London to Asia, then the last flight out of Asia to New Zealand. Crisis averted, she thought.
She moved in with her parents in Auckland, continued studying towards her master’s degree over Zoom in the evenings—what passed for normal in 2020. She got a job, joined a gym. Six months after her return, her grandfather died, and her grief took the form of a brutal, relentless insomnia. And then the virus came back again—or that’s what it felt like. It was almost as though she’d caught COVID-19 a second time: the aches, the shortness of breath, the sore throat. She even went and got a test, but it was negative. The main difference was that this time, she didn’t get better.
When Orgias saw her doctor, it was physically difficult just to explain what was happening to her body. “Talking to her in her office, I was hyperventilating, I was struggling to get breath,” she says. She was perpetually exhausted, sleeping until 4pm each day, then going back to bed at 10pm. Her heart rate would spike at random times, pounding hard in her chest.
The doctor referred Orgias to a breath specialist, who found her lungs were functioning at 30 per cent of a normal person’s capacity—and Orgias, a soprano, should have had the lungs of an elite athlete. That probably explained, she thought, why she’d become unable to sing.
[chapter-break]
Connor Mitchell had been at university in Christchurch for only a couple of weeks when the first nationwide lockdown was announced on March 23, 2020. Now the lecture halls were closing, classes were going online, and people in his hall of residence were leaving one by one. It felt a little bit apocalyptic, and a little bit like Christmas, everyone going home for the holidays. Even his brother had cut short his travels and flown home. Mitchell left Christchurch and arrived at his parents’ place north of Wellington just after his brother tested positive for COVID-19. Mitchell, his mum, and his brother’s wife also came down with it, but Mitchell, the youngest member of the household, got it worst. He lost his senses of smell and taste, and the passages of his nose and throat felt raw. It hurt to breathe. Fevers came and went.
After about three weeks, he turned a corner. It felt as though his body regrew his taste buds.
“I thought that was over and done with,” he says. “But then I started noticing being completely fatigued. I’d get really lightheaded, almost like tunnel vision, whenever I tried to do exercise.”
He picked up his university work again, but all of a sudden, it was harder. “I’d find myself writing a full paragraph and then reading it back and it wouldn’t make sense, and just clearly something wasn’t working in my brain,” he says. “I had assignments that I just didn’t do because they were based on a computer, and at the time, my vision wasn’t up to reading off the computer.”


When lockdown ended, Mitchell returned to Christchurch, but he wasn’t well. Getting through the day required a titanic effort. “It was really weird just trying to get over the fact that I couldn’t function normally, especially being, at the time, 18, a fit male, I always felt like I could achieve everything that I needed to if I put my mind to it. Having this physical block really put me in a bad spot. I struggled quite a bit with that, just having to recognise that I had a limit all of a sudden.”
He rationed visits to the doctor: a walk across the campus to the clinic would wipe him out for the day. He was sleeping from 9pm to 2pm, and in his small window of wakefulness applied himself to his studies with a ruthlessness born of desperation. He just had to knuckle down, he told himself, and get through to the second year of his degree, even if it cost him his mental health. “I passed all my courses that I had to,” he says, “but I had a pretty horrible time doing it.”
In the end, Mitchell’s grades weren’t high enough to gain automatic entry into his second year, and he wasn’t able to get any kind of compassionate consideration for his illness. He faced a long wait over the summer holidays to see if he’d be allocated a place.
[chapter-break]
Mitchell is officially regarded as “recovered” from COVID-19—but, like Orgias, Brown, and Robb, he isn’t exactly better. All four have ongoing health problems that they’d never experienced before their infection. All of them have an illness that much of New Zealand, including the government, is yet to acknowledge: long COVID.
Long COVID is one of the pandemic’s biggest mysteries. We don’t know how many people will develop it—it’s thought to be around ten per cent of unvaccinated cases, but it’s difficult to measure, as some people’s symptoms, like Orgias’s, don’t kick in for several months. We don’t know how much vaccination reduces the likelihood of developing long COVID: one study estimates that vaccinated people who come down with the virus are about half as likely to feel sick four weeks later as unvaccinated people, though this doesn’t take into account the fact that many long COVID symptoms begin many months down the track. And we don’t know who among us is susceptible to long COVID, or why. It strikes the healthy and young as well as people with compounding medical conditions.
In other words: we can tell who in a population is most likely to die of the virus, but we can’t tell who is most likely to get terribly sick. This makes catching the coronavirus like entering the world’s worst lottery. If you win, you get your normal life back—and there’s a big chance you will win, perhaps as high as 90 per cent. But if you lose, the virus will change your body, and it may do so permanently.
When New Zealand Geographic first described scientists’ predictions of New Zealand’s worst-case scenario—a massive COVID-19 outbreak—it involved thousands of deaths and an overwhelmed hospital system. As we’ve learned more about the virus and the trail of destruction it can leave, we can add an extra detail to the worst-case scenario: tens of thousands of New Zealanders who don’t get better, who can’t work or care for their family members, and who are struggling with the loss of most of the things they enjoyed in life.
[chapter-break]
So, what to do about COVID-19? Until the Delta outbreak, New Zealand’s strategy was clear: the virus wasn’t allowed into the country. The government developed a plan to unfurl the country little by little once it had the tools to keep the virus at bay: vaccinations for everyone over the age of five, at-home tests that give results in 15 minutes, new medications to treat COVID-19, improved ventilation in buildings, more information about which members of the population are most at risk, and a better idea of the long-term burden of the virus.
Unfortunately, the plan didn’t have a section on what to do if the virus leaked out of managed isolation and quarantine (MIQ) facilities and began spreading all over Auckland before the government had acquired more of those tools for controlling it. “Somehow we’ve got to transition to the kind of longer-term strategy on which there was a lot of work done,” says Shaun Hendy, a University of Auckland physics professor who has been modelling the pandemic since its outset with a team at Te Pūnaha Matatini research centre. “But it’s all predicated on putting that strategy in place with basically zero or very small case numbers.”
[sidebar-1]
Eliminating the virus from New Zealand, says Hendy, is now out of our grasp: “We’ve just run out of shots to fire.” The virus got around our Alert Level 4 defences, largely thanks to some of New Zealand’s other issues: overcrowded housing and people experiencing homelessness. “It’s highlighted some long-standing problems that we’ve not dealt with.”
There are a couple of other options for controlling the virus, says University of Otago epidemiologist Michael Baker, who advises the government on its COVID-19 response. Baker is widely credited as the architect of the elimination strategy that New Zealand has followed until now.
[chapter-break]
The first option is “suppression”. We could decide to block the virus, to tackle it whenever it tries to run away, to hamper it from spreading freely—and to stop it getting to people or communities at risk. Suppression can be strict or mild, but either way, it would involve changes to daily life especially designed to stop respiratory viruses from getting around.
Many of the changes would involve indoor spaces. We would need to become obsessed with the cleanliness of the air we breathe, in the same way that we are about the cleanliness of the water we drink. That means ventilation systems would need to be improved everywhere.
“It’s one of those things that seems expensive, but it’s actually cheap compared to lockdowns and compared to the health impacts of the virus,” says Michael Plank, a mathematics professor at the University of Canterbury who also works on pandemic modelling. “So actually investing seriously in ventilation and air filtration is going to be worthwhile in the long run. It doesn’t require any behavioural changes, and it has other benefits as well—having good air quality reduces the transmission of other respiratory pathogens like seasonal flu.”
It’s possible to create safe indoor spaces. The virus doesn’t appear to spread as readily on aeroplanes as it does at indoor parties. Long-haul flights may be cramped, but they’re extremely well ventilated. On the other hand, crowded spaces where people have to shout to be heard or are heartily singing are high-risk situations for contagion.


Improving ventilation in schools is particularly crucial, because children under 12 aren’t presently able to be vaccinated and could form an ever-circulating pool of transmission. “Although young kids are at relatively low risk of getting seriously ill, they can still suffer from things like long COVID,” says Plank. “They can also act as a sort of a conduit that allows the virus to spread to other age groups, and so it can have indirect consequences for others in the population, if you have high infection rates in children.”
The Australian state of Victoria recently bought 51,000 air purifiers with high-efficiency particulate air filters—the type used in hospitals—for its schools. These HEPA filters strip the vast majority of viral particles from the air. The schools will keep track of air hygiene with carbon-dioxide monitors, which indicate whether a room is stuffy, requiring either more ventilation or fewer people using it.
On a personal level, mask-wearing would continue in high-risk situations, such as on public transport and around vulnerable people. Regular testing would become a habit—not the uncomfortable up-the-nose PCR test, but do-it-yourself tests that show the results immediately. People would take rapid tests if they felt unwell, and before they went to places known to be high-risk, such as hospitals or aged-care facilities or music festivals. They would also need to take tests on a random, regular basis—about 50 per cent of coronavirus transmission is thought to come from asymptomatic infections, so halting the virus means keeping an eye on healthy people as well as sick people.
Rapid tests are less accurate than PCR tests, so a person who tested positive would then take a PCR test to confirm the diagnosis.
The outdoors will be fine, because the virus is generally swept away in fresh air. Perhaps there would be a shift in how we socialise inside, in restaurants and bars. Perhaps city regulations would relax in order to allow outdoor seating. We would have a whole summer to figure out how to translate the new norms of socialising and dining into winter.
With suppression, the big question is: which health measures walk the ideal balance between the terrible impacts of restriction—the loss of many things that make life meaningful—and the protection of people from an illness they wouldn’t wish on their worst enemy?
[chapter-break]
The other option for New Zealand is “mitigation”, which involves letting the virus go wherever it wants, but taking enough action to prevent the country’s health system from being overwhelmed. The main tool for this strategy is vaccination, as this reduces the chance of a person being hospitalised or dying by around 90 per cent, and also reduces the rate of transmission.
While vaccinated people can be just as contagious as unvaccinated people, they are less likely to pass on the virus to others, according to a growing body of research. It’s counter-intuitive, but this is probably because vaccinated people clear the virus more quickly from their bodies than unvaccinated people, meaning they’re infectious for a shorter period of time.
For vaccination to work well as a form of protection, vaccination rates need to be similarly high throughout a community. This is why national vaccination rates can be a poor predictor of cases and hospitalisations. A high national average may conceal big peaks and troughs in vaccination rates: 99 per cent coverage in some areas but 15 per cent coverage in other groups, for instance. Unvaccinated people are best protected when they are sprinkled around a population of vaccinated people. In reality, unvaccinated people tend to form communities, and the virus seeks these out.
[sidebar-2]
Mitigation is the United Kingdom’s strategy. If New Zealand adopted it tomorrow and it had the same effect here, once the virus got up to speed, around 10 people would die from the virus each day—around 3500 additional deaths a year. (By comparison, about 500 people die of influenza each year.)
That said, the United Kingdom has previously had large outbreaks of the virus, so its population has a higher level of immunity than New Zealand’s does.
“We haven’t been through that ordeal that they had in much of the world,” says Baker, “where it just swept through societies and hospitalised a lot of people and killed a lot of people.”
In other words, the rate of deaths and hospitalisations here would almost certainly be greater than in the United Kingdom.
In the end, the government may not have much of a choice. The door to the path of suppression is closing with the rise in case numbers. If these aren’t low enough, then typical suppression measures won’t keep them in check, and the country is left with mitigation, or “stop the health system from becoming overwhelmed”.
Hendy describes mitigation as “an ‘Alert Level Three forever’ option”. If cases continue to increase, this will lead to a large outbreak over the summer. “To keep things anywhere near our healthcare capacity—and we probably won’t—we’re going to have to stay in quite a stringent lockdown for an extended period of time,” he says. “I think we’re just on the threshold—it could go either way at this point. There’s a bit of a strategic gap, as I see it. This kind of situation hasn’t really been planned for.”


What would wide transmission look like in New Zealand—and what would be the consequences of it? We just don’t have the right information to figure this out.
“The biggest missing element, I think, is long COVID,” says Baker. “So do children also get these long-term effects in even remotely similar ways to adults? And we don’t know how long it will persist for. Even if it occurs at the level of down to one per cent, that would still be a major burden.”
Moreover, a significant question still circles around vaccination: how safe is it to meet the virus once you’re vaccinated?
“It may be that this is a virus that you never want to be exposed to even if you’re vaccinated,” says Baker. “For me, that’s a great unknown.
“I think sometimes the government would like to think, ‘Oh, we could just vaccinate our way out of this’, but unfortunately, it’s not true.”
[chapter-break]
In the meantime, New Zealand scientists have set out to address one of those unknowns: who gets long COVID, and why?
“The thing is, this was completely predictable,” says immunologist Anna Brooks. “And the thing about long COVID is that it’s not a completely new phenomenon. It’s not a mystery disease. It’s none of those things. It’s a post-viral condition.”
Scientists have known for a long time that some people who catch viruses don’t recover—for months, or years, or at all. These conditions have a variety of types and names: myalgic encephalitis (ME), also called chronic fatigue syndrome (CFS), or post-viral syndrome, or sometimes they have no name at all. The lingering illness that struck flu survivors after an outbreak in Tapanui, near Dunedin, in 1982 never got an official title. (There are perhaps 75 outbreaks known to have caused residual long-term illness.)
There are a few ideas about what causes long-term illness after a person recovers from a virus. Perhaps someone’s immune system goes into a frenzy and starts attacking their own body with friendly fire once the virus is defeated. Or perhaps their body is too weak to tidy up the damage that the virus has caused, and there’s smashed-up bits of virus all over the place—the residue of the battle.
“When a virus infects a cell, the immune system kills the cell, so there’s just garbage everywhere,” says Brooks. “We think of it as areas in the body that have debris from the viral infection triggering the immune system. Basically, anything foreign in your body is going to keep the immune system active.”
Or perhaps the virus caused such massive disruption that the body hasn’t been able to heal yet, and that healing process is measured in months or years rather than days.
“Some people might have long COVID for six to nine months and get better,” says Brooks. “And maybe it just takes that long for the immune system to calm down from the terrific attack it had.”
The most common symptom that people experience is fatigue: their body shuts down and goes into recovery mode, unable to perform anything above the most basic functions. (“It’s just like being on life support,” one medical professional who has ME told me.) It often arrives late, and with a different set of symptoms from the person’s initial bout with the virus.
“The more you talk to people with long COVID, the more you understand that someone’s long-COVID symptoms are unpredictable and could kick in at six months,” says Brooks. “So they might think, ‘Oh, you know, I’m getting through this.’ And then a bunch of new symptoms kick in, because we just don’t understand the extent of what this virus has done.”

Unfortunately, we haven’t got very far in measuring exactly how many people are experiencing this. Because of this, we don’t know what a person’s likelihood of getting long COVID is, and we don’t know how those odds change across age and ethnicity. If we knew, we might be able to prepare for the challenges that thousands of New Zealanders are likely to face. “This isn’t unique to New Zealand,” says Brooks. “No government anywhere in the world—no ministry—is tracking people who don’t recover from COVID.”
Most countries haven’t been able to keep track of their total number of COVID-19 cases, but New Zealand has. Now, Mona Jeffreys and Lynne Russell of Victoria University are going to have a shot at figuring out exactly how many people are still sick. They’re aiming to get in touch with everybody in the country who’s had COVID-19 to ask them about any long-term symptoms, any challenges they had obtaining a diagnosis, the barriers they’ve faced in getting care, and the kinds of services that might have helped with their recovery.
[sidebar-3]
The two researchers have designed their study with input from the 250-person long-COVID support group on Facebook, and Jeffreys hopes to get a clearer picture of the severity of ongoing symptoms. “If you have a persisting symptom that’s fairly mild, that’s completely different to people who are bed-bound,” she says. “And I think that’s really important for us to get a really good handle on, because it makes a huge difference, obviously, for individuals, and also for predicting health service needs.”
Jeffreys also has ME, triggered by a stomach bug years ago—“something you wouldn’t think twice about normally”. She has ticked off many items on the bingo card of terrible medical experiences: being told she was making up her fatigue, or being told there’s nothing that can be done for her. “We know that isn’t true, because there’s very good evidence for things that can help for ME.” And now, some of those things might help long COVID, too.
Biochemist Warren Tate, an emeritus professor at the University of Otago, has identified molecular differences in the immune systems of people with ME—different amounts of proteins involved in energy production—and is now undertaking the same investigation with people who have long COVID.
“We’re looking to see, does long COVID have the same molecular signatures?” he asks. “Or does it have different ones? So, to see whether it’s a very similar kind of disease, or whether it’s a sister disease with its own unique characteristics.”
Meanwhile, Brooks has been crowdfunding to launch her own research project into what happens in the immune systems of people with long COVID. She’s going to analyse what’s happening in the cells of people who’ve had COVID and recovered, people who are living with long COVID, and people who have been vaccinated against COVID, with the aim of pinpointing what’s different about their immune responses. Is there a clue there that may tell us who’s susceptible to long-term illness? “The critical thing about our immune system is that it remembers, so we should be able to find evidence of that memory,” she says. “One potential reason that people get post-viral conditions is that they didn’t have the right kind of immune response or a strong enough response to get the job done. Or their immune system misfires, and then remains stuck in a disrupted state. We don’t know.”
[chapter-break]
Luke MacLean-McMahon sets four reminders for our Zoom meeting, such is the level of memory loss and brain fog he experiences. One of the symptoms that affects him most these days is blackouts—before we spoke, he blacked out while on a walk. He’s been diagnosed with long COVID, dysautonomia, chronic fatigue, heart damage and post-traumatic stress disorder (PTSD)—but specialists are still trying to figure out the cause of the blackouts. He sometimes feels them coming on—“It’s quite blurred vision, things just start going a little buzzy”—and if he does, he can get down on the ground before he loses consciousness.
MacLean-McMahon is in his early 30s, and he used to exercise six days a week. The dramatic change in his capabilities has had a huge impact—he’s lived with the aftereffects of COVID-19 for 18 months and counting. “I’ve struggled possibly more on the mental side than I have on the physical,” he says.
He’s grappled with anxiety, with depression, insomnia and with PTSD. He can’t forget what he saw while in hospital with COVID-19 in London, surrounded by the very ill. Nor can he forget the impact the pandemic has had on the nurses and doctors he got to to know—“hospital heroes”, he calls them.
He’s had to adjust his idea of personal victories—walking up a steep street now in Auckland without stopping is an achievement. Now, he aims to walk a half marathon one day.
Similarly, Connor Mitchell says the experience of long COVID has led him to question his identity. “I was always pretty tough on myself academically and physically, and I put a lot of my self-worth into those things, and then as soon as I couldn’t do certain things, I took that really tough—and I was kind of searching for what I was doing, or just why I was me.”
Mitchell was eventually accepted into the second year of his degree, and he thinks his brain is slowly returning to its regular speed. “I’m not sure, because it’s been a year and a half since I thought normally,” he says. “It’s hard to remember what you used to think like.”
Christina Orgias, the soprano, wasn’t able to sing for a year, but she’s just been able to start again—the result of regular breathing exercises to improve the strength of her lungs, and a strict protocol to manage her postural orthostatic tachycardia syndrome, or POTS. When her heart began to race at random times, she learned to stop everything and sit down until it settled down. “When your heart is up there all the time and you’re not even doing anything, your body thinks it’s in stress mode all the time,” she says, “so therefore it’s not in healing mode. It’s in fight mode.”


It was tremendously frustrating to have to continually pause and rest, but after a couple of months’ careful attention to keeping her heart rate down, she began to feel different. These days, she wakes up at 1pm rather than 4pm, and slowly, she’s living up to the encouragement of her breath specialist. “She said to me, it would be a long time to get back to where I wanted to be, but she said, ‘You can 100 per cent get back.’ She said, ‘It’s a long game. But it’s completely doable.’”
Orgias knows that she’s lucky to have a doctor and a specialist who identify her illness as long COVID; others, such as Sue Robb, the veterinarian, struggle for recognition and care.
“I’m sore,” says Robb, matter-of-factly, when I ask how she’s doing. She’s also lacking an advocate within the medical system to fight for the right treatments for her. The experiences she recounts having with health professionals are alienating rather than affirming.
Geoff Brown, who spent almost a week on his bathroom floor, successfully protected his family from the virus: no other members of his household tested positive. Eighteen months later, specialists are still trying to decipher the new irregularity of his heart. He wishes he’d sought medical help more quickly when he first got sick, but no one he spoke to at the time seemed to think he needed assistance—he didn’t even need a test—and he has the politeness of his Samoan culture. It wouldn’t be like him to force the issue.
He wishes someone had told him not to push himself to go for walks after getting home from hospital—he thought forcing himself to exercise would help him recover, but instead, it precipitated a relapse. “I know today that you’re supposed to rest up; you’re not supposed to exercise after COVID-19 because you’re just fuelling your heart rate,” he says. “You’re actually adding to your recovery.”
[chapter-break]
So far, in New Zealand, we’ve been fortunate to have avoided the tolls of COVID-19: illness, death, disability, and the long disruptions to lives and relationships, education and work. But now we’re entering a new and dangerous period, where our freedom is finely balanced with the unknowns of this mercurial virus. Some of those unknowns may take years to unpick. Others are being actively studied or documented overseas.
New Zealand has the advantage of being further back in time than other nations, with more of the tools—mostly in the form of vaccinations and information—than other governments had when faced with uncontrolled outbreaks. We know about the effects of unvaccinated populations, the half-life of vaccines and the explosive infectiousness of Delta. Add to that our biggest known unknown—the spectre of long COVID, which may well be the ghost that haunts us long after the outbreak has waned.
The power of R
The incredible virality of Delta can be explained mathematically. The first strain of COVID-19 to emerge from China had an R value of around 2, meaning that each host infected around two others. They infected two others, and so on, so that after four transmissions an epidemiologist might expect 16 new cases for a total of 31 in the outbreak.
Consider, however the Delta variant of COVID-19. There is nothing magical about this pathogen except that its hosts carry a higher load of the virus in their throats and nasal passages (as much as 1000 times higher), and therefore have more to share around. This results in an R value of greater than 6. At face value, this might appear to be three times worse than the original strain, but humans are not good at appreciating the power of exponents.
If one person passes the virus to six others, and each of them to pass it to six others, after four transmissions there are 1296 new cases and 1555 in total. One more transmission results in 7536 additional cases, then some 45,000.
The serial interval—the time between transmission and the new host becoming infectious to transmit it again—also appears to be short with Delta; four days to the original variant’s seven, meaning it could infect some 280,000 in the month that it took the 2020 virus to infect 31.
The only defences are vaccination, or reducing contact between individuals.

Lockdown-o-meter
We haven’t had it so bad. A ‘stringency index’ is a composite measure based on nine response indicators including school closures, workplace closures, and travel bans, rescaled to a value from 0 to 100, where 100 = strictest. (If policies vary at the subnational level, the index is shown as the response level of the strictest subregion.) It’s a graphic demonstration that the ‘hard and early’ approach has meant much greater freedoms than enjoyed in other countries.
DATA: Oxford COVID-19 Government Response Tracker, Blavatnik School of Government, University of Oxford — ourworldindata.org/coronavirus

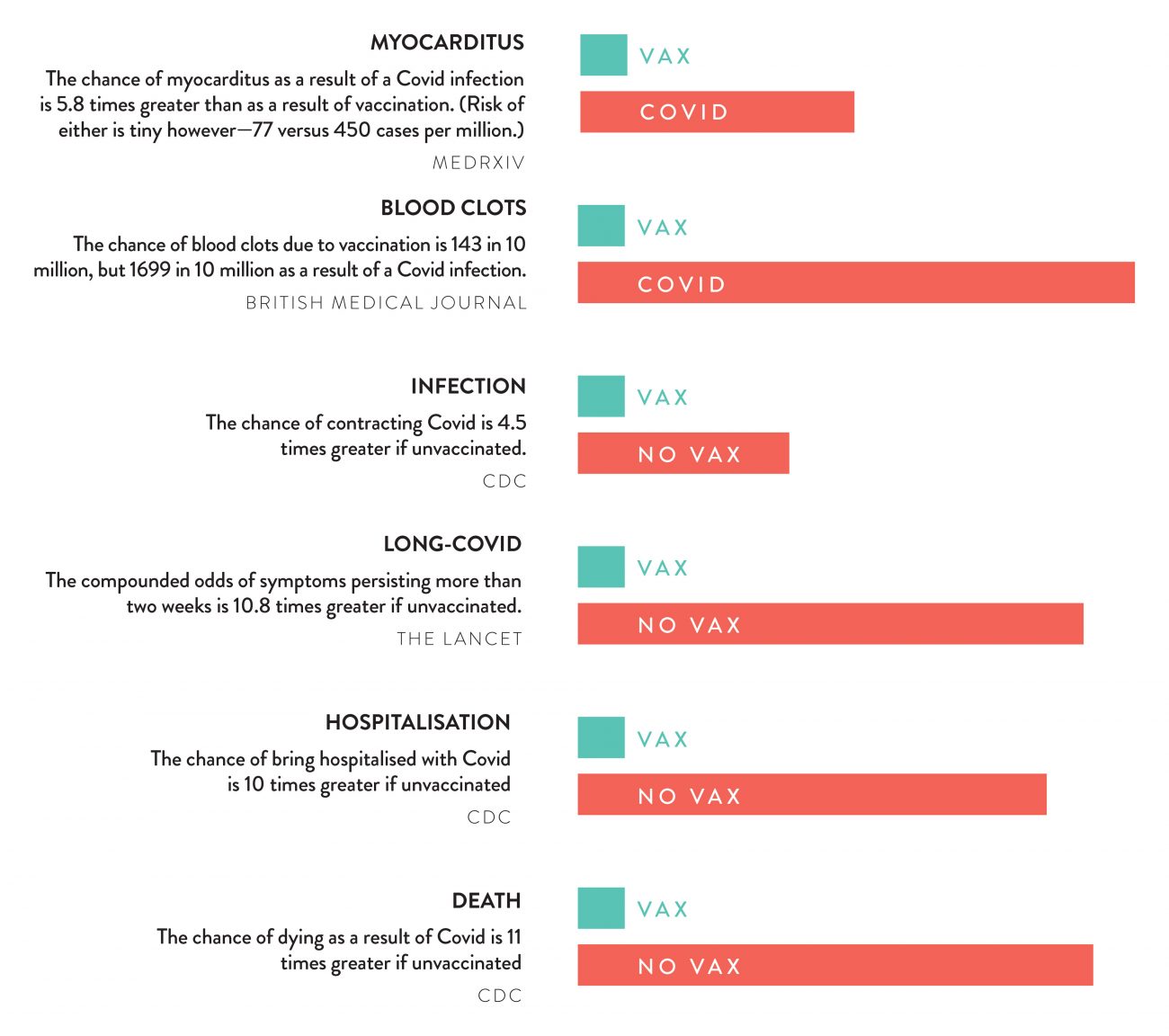
What are the chances?
Percentages and compounding odds can be difficult to understand. Here we break them down. The misinformation mill has made much of the risk of myocarditis as a possible side effect of vaccines. Those who receive the vaccine have an elevated risk of myocarditis, or heart inflammation, but it remains small—77 in a million. And if infected with COVID-19, those odds increase 18.2 times, to 450 in a million. Likewise the odds of blood clots. Likewise the odds of long COVID, hospitalisation or death. Those without vaccines are 4.5 times more likely to contract COVID as the vaccinated, and less protected if they do. No one wants a jab—but how lucky are you feeling today, exactly?